Overview of Achondroplasia
Achondroplasia is the most common type of skeletal dysplasia and accounts for nearly 90% of disproportionate short stature or dwarfism. Characterised by impaired endochondral bone growth, it is caused by a gain-of-function mutation in the fibroblast growth factor receptor 3 (FGFR3) gene.
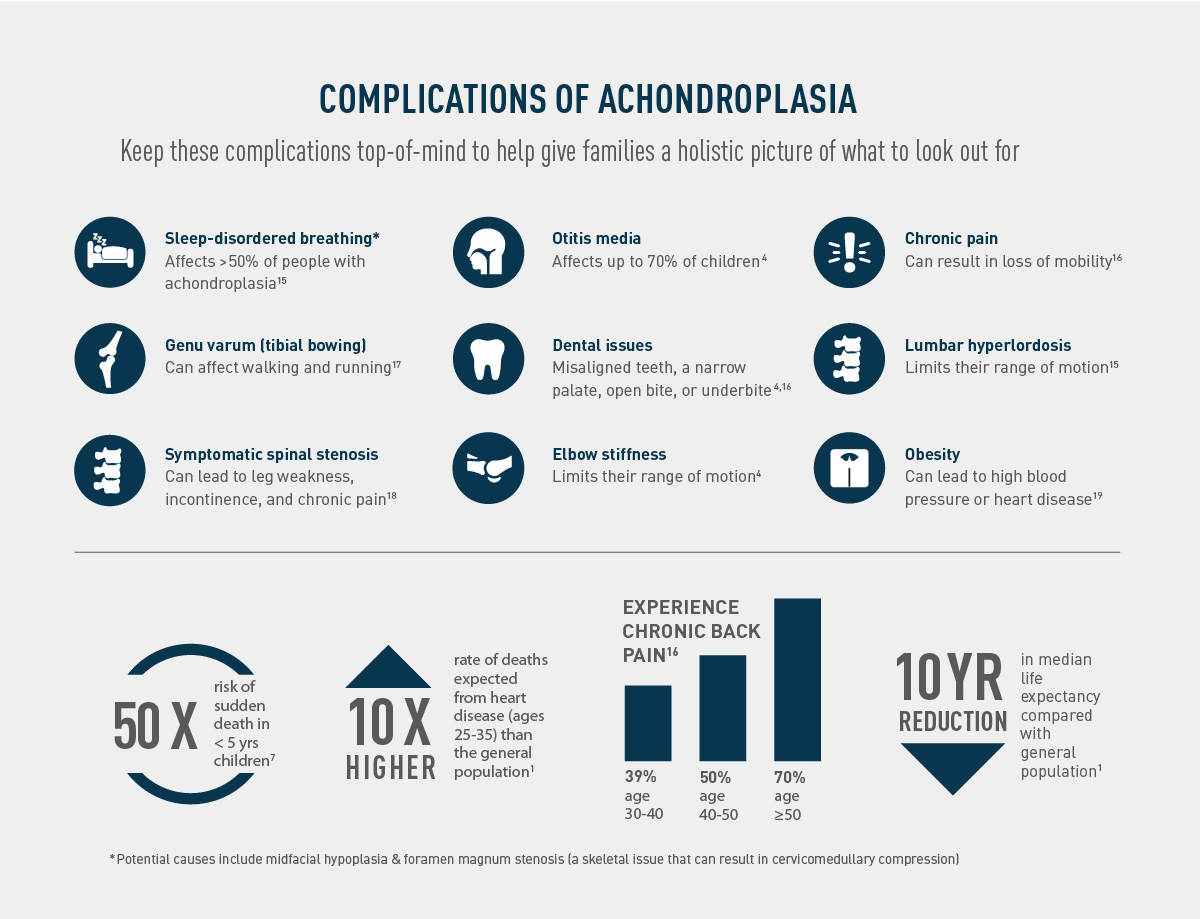
References:- Ireland P et al. Optimal management of complications associated with achondroplasia. Appl Clin Genet 2014;7:117-25
- Horton WA et al. Achondroplasia. Lancet 2007;370:162-72.